One of the most common situations in my practice is that people arrive preoccupied having performed an analytical and note that your total cholesterol is over 200, either because they are alarmed or because the doctor shared that concern.
In most cases, there is no cause for alarm. However, it is often a challenge to convince them of the biomarker of ‘total cholesterol’, by itself, does not provide much information about its cardiovascular risk. The issue is much more complex than simply observe this value and ‘to bring’ the issue. For example, there is a molecule that is strictly correlated with the cholesterol, APOB, which offers us much more detail. In addition, other indicators, such as triglycerides, glucose, insulin, and homocysteine, also provide relevant data on the cardiovascular risk. Even in contexts appropriate, a total cholesterol level above 200 it may be more beneficial and protective to harmful.
Given the importance and widespread confusion on this subject, in my book Feeding Evolutionary dedicated a chapter unique to him. As yet there are those who have not read, and, considering that the topic may sound like something technical and complex, to those who have already done that don’t would be nice to cool it. That’s why I’ve decided to write an article on the blog.
So, let’s clarify what we are talking about when we refer to cholesterol, to demystify the idea that there is something harmful in itself for the health and stripped of the role of ‘bad guy’ in coronary heart disease.
We begin with the following statement:
Without cholesterol we die
As simple as that.
Why do we need cholesterol?
- An essential part of all of our cell membranes, giving them waterproof and integrity.
- It is necessary to produce bile, which is essential to the digestion of fats and the vitamins associated with (A, D, E, and K).
- Participates in the production of sex hormones (testosterone, estrogen, progesterone) and adrenal (cortisol, aldosterone).
- Forms part of the myelin sheaths that coat the axons of neurons, which is essential for their connections, their function and the transmission of the nerve impulse, as well as for motor activity and intellectual.
- It is essential to synthesize vitamin D. The deficiency of this vitamin means there is a greater risk of developing colon cancer and breast cancer, infections (including covid-19), diabetes (both types), asthma, osteoporosis, rickets, autoimmune issues, multiple sclerosis, thyroid dysfunction, inflammation, obesity, or hypertension.
- Helps to repair the wounds that may form in the blood vessels by inflammation and oxidation, in turn caused by high levels of glucose.
- It is critical for the function of the neurotransmitter serotonin, which, among other things, keeps the mood.
Do you have to have it the lower the better?
Well, NO.
Try to reduce the cholesterol to a minimum to reduce the cardiovascular risk is as forbidding the circulation of cars on the roads to prevent traffic accidents. Cholesterol, like the cars in the accident, the cause is necessary, but not sufficient, for cardiovascular disease.
There is a general belief, promoted by media, some informed and some health professionals outdated, that cholesterol should be kept as low as possible. This is not true. As we mentioned, the cholesterol is essential for life; without it we could not live. Therefore, something that is essential for life may not be inherently bad, and reduce it to a minimum is not only beneficial, but they can be harmful. As in many aspects of life, the body needs a balance (homeostasis) in order to function properly. Both the excess and deficit are harmful.
By way of example, a meta-analysis of 2016 of the University of South Florida, which included 19 studies with 30 groups and around 68,000 participants from more than 60 years, showed that people with high levels of LDL cholesterol (the supposedly ‘bad’), lived longer, or at least equal, than those with low levels. Specifically, 92 % of the cases, there was an inverse association between all-cause mortality and high levels of LDL; in the other there was no relationship. The authors concluded: ‘Our review has shown a lack of association, or even an inverse association between LDL-C and mortality from all causes and due to cardiovascular disease‘.
Other studies support this idea, suggesting that an LDL relatively high, which may protect against diseases such as cancer and certain infections, while an LDL low may increase the susceptibility to these diseases. It is important to point out that, when we refer to ‘high levels’, we do so in relation to the ranges ‘official’ common, they are lower than they should be; we do not speak of levels excessively high, which themselves may be harmful.
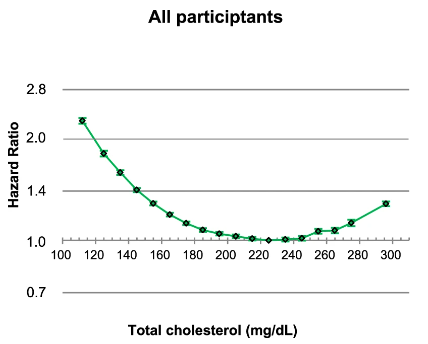
In a meta-analysis of 2008, carried out by japanese scientists to relate the level of total cholesterol with all-cause mortality, it was concluded that people with total cholesterol below 160 mg/dL had the highest mortality, whereas those with levels between 200-240 mg/dL were the most long-lived. That is to say, the lower the cholesterol, the greater the risk of death. Another study comes to the same conclusion: lower all-cause mortality with levels of total cholesterol between 200 and 240 mg/dL.
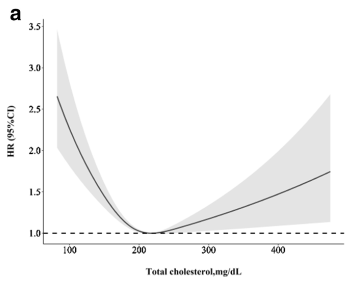
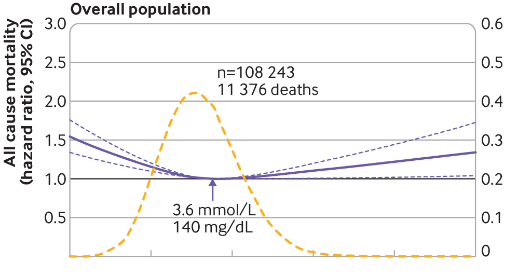
I don’t want to aburriros with more studies, but I promise you that this is the last. Published in Nature in 2019, with nearly 13 million cases analyzed, confirming that the levels of total cholesterol and all-cause mortality followed a curve in the shape of a U. The ‘sweet spot’ of lower risk of mortality is between 210 and 250 mg/dL, with an equal risk of mortality to 270 mg/dL (something that escandalizaría to a conventional doctor) to 170 mg/dL (level that a doctor would consider to be perfect). The Spanish Social Security states that the total cholesterol should always be less than 200 mg/dL. No comments.
With the LDL-C something similar happens with the ‘sweet spot’ of lower mortality from any cause between 100 and 160 mg/dL (study, study).
Now that we know that it is not beneficial to maintain the cholesterol as low as possible, and that the ranges officials have no solid scientific basis, those who are curious can continue reading to better understand what we mean when we talk about cholesterol.
What is cholesterol?
Cholesterol is a molecule essential for life, the body (specifically the liver) occurs in the quantity you need. This endogenous production is complemented with the cholesterol we ingest through food, although the latter contributes a lot to a lesser extent. The liver produces daily between 1.5 and 2 grams (the equivalent of which contain 7 to 10 eggs); to stop eating eggs will not lower your cholesterol, as if we consume less, the liver will compensate by producing more.
To be hydrophobic (such as whole fat), the cholesterol molecule cannot circulate freely in the blood (which is roughly a 50 % water). Therefore, in order to be able to travel through the blood circulation and reach where it is needed, you must join a few particles called apolipoproteins, thus forming the well-known lipoproteins (which are measured in the conventional analytical). These lipoproteins, as their name suggests, they are composed of lipids (cholesterol + triglycerides) and proteins (apolipoproteins).
There are several types of lipoproteins according to their density, but, to simplify, let’s talk only of the two most well-known and that we measure in the analysis: HDL and LDL. The density refers to the ratio protein/fat; that is to say, the more protein (and less fat) have the lipoprotein, the greater will be its density and smaller it will be.
- HDL: acronym in English of high-density lipoprotein (high density lipoprotein), known mistakenly as ‘good cholesterol’. 50% of its composition is protein and 50 % fat. Binds to apolipoprotein A100 (APO A1). Its main function is to collect the cholesterol (and other fats) left over from cells and carry it to the liver for disposal.
- LDL: acronym in English of low-density lipoprotein (low density lipoprotein), so-called ‘bad cholesterol’. It is unfair to call it ‘bad’ to a particle necessary for life and with a primary function. The 20 % of its composition is protein and the other 80 % fat (of which 80 % is cholesterol and 20% triglycerides). Binds to the apolipoprotein B (APO B) and carries cholesterol to the cells for use.
To better understand how all this works in our body, imagine a set of trucks of various types (lipoproteins (HDL and LDL) loaded with goods (cholesterol + triglycerides). Trucks LDL transport goods to its destination (the cells) for its use, while the trucks HDL collect the excess goods and carry it to another destination (the liver) for recycling. All this happens through a highway (the blood) that circulates within a few tunnels (the blood vessels), and as the whole tunnel, have walls (endothelium).
What we measured the conventional analyses?
Triglycerides
Are all fats that carry our lipoproteins in the blood. When there is an excess of carbohydrate in the diet and consume more of what we spend, the deposits of glycogen to fill up quickly. The hormone insulin —our body does not waste anything, because they do not know when we will return to eat— stores this excess carbohydrates in the adipose tissue, pre-transformation into fat. Unlike cholesterol, triglycerides, have a primary function: to be stored to be used as a source of energy when we do not receive enough food. However, when these triglycerides are elevated (>100 mg/dL), acquire an inflammatory action and increase the cardiovascular risk.
Total cholesterol
Includes all types of cholesterol (the ‘goods’) that transport lipoproteins (the ‘truck’ delivery and pick up) by the blood (‘highway’). To assess the risk of coronary or cardiovascular, this value provides very little information.
HDL-C
Corresponds to the total cholesterol-carrying lipoproteins (HDL in the blood, with the aim of recycling in the liver.
LDL-C
Is an estimate of the total cholesterol-carrying lipoproteins LDL in the blood to carry him to the cells. I say ‘estimate’ because not even be directly measured (it is very costly to); instead, it used a formula of Friedewald, which dates back to 1972 and is out of date for individuals with triglycerides under 100, because it overestimates the amount of LDL. It is more reliable the formula ‘iranian’ in 2008, although it is still used in our health care system. This data (I repeat, estimated) considers only the total amount of LDL cholesterol that circulates in the blood (the ‘goods’ LDL total for the ‘road’) and not the number of particles (this would be the LDL-P, not LDL-C) or lipoproteins (the ‘trucks’) that are circulating. Is not the same as all merchandise trip in a lot of ‘truck’ small that few but large. Later we will see that knowing the amount of trucks/lipoprotein LDL circulating cholesterol (LDL-P) is more relevant to know the total of the goods/cholesterol-carrying particles, LDL cholesterol (LDL-C), which is what normally measured in the conventional analyses.
We can distinguish two types of lipoproteins LDL according to their size:
- Large (diameter >26 nm) and ‘fluffy’, which are harmless. After 2-5 days, return them to the liver for recycling after fulfilling their function of transporting cholesterol and triglycerides to the cells.
- Small (diameter <24 nm), ‘dense and hard,’ which are dangerous. These particles damage the arterial wall or endothelium (the ‘wall of the tunnel’) when they are glicadas by glucose and oxidized by an excess of free radicals in an environment prooxidant: tobacco, stress, high levels of blood glucose, consumption of trans fats/hydrogenated fats, sugar, diet poor in antioxidant, excess omega-6, and deficit of omega-3, among other factors. In addition, the smaller the particles, LDL, the greater will be their ability to pass through the endothelium, embedded in him and begin to form the atherosclerotic plaque.
The danger for cardiovascular: atherosclerotic plaque. How to form?
The danger begins when they accumulate triglyceride and LDL-cholesterol, oxidized. This attracts monocytes and macrophages, which promote inflammation and damage to the collagen layer of the endothelium of the blood vessel, facilitating rupture and allowing the lipoproteins LDL from small size to pass through more easily. In response to this rupture, platelets, and fibrinogen to accumulate, forming a thrombus (blood clot), which can obstruct the blood vessel (the ‘tunnel’), increasing the risk of a stroke by blocking the circulation and prevent everything necessary to arrive at your destination.
The calcification of the arterial tissue is part of the healing process; therefore, a good test to evaluate the cardiovascular risk is to measure coronary artery calcification.
As I already mentioned, is not the same as the same amount of goods to be transported for many ‘truck’ little by little ‘truck’ big. With many small trucks, there are more ‘circulatory’. In addition, only small trucks can pass through and embedded in the hollow of the damaged wall of the tunnel.
Therefore, in order to know our true cardiovascular risk, what is of interest is the size of our LDL. The ideal thing would be to measure the actual number of particles LDL circulating cholesterol (LDL-P) and not only the total amount of cholesterol that transport cholesterol (LDL-C, which is what is usually measured in the laboratory tests). This is because, for the same amount of total cholesterol, if there are few particles, these will be larger (the same ‘commodity’ carried by a few large trucks) and not cross the endothelium, thus preventing the formation of the atherosclerotic plaque and, thus, reducing the risk of heart disease. In the end, that is what really matters when you control your cholesterol levels.
How to know the actual number of lipoprotein LDL (LDL-P) that we have in the blood to estimate your size)
For now, you can only determine through the use of technology of nuclear magnetic resonance (NMR) or by electrophoresis, both techniques are costly and still not 100% accurate.
What other alternatives more affordable exist?
Measure the APO B
Recall that the cholesterol carried by the particles LDL is linked to the apolipoprotein B (APO B), and that 90% of the APO B in the body comes from the LDL. Therefore, knowing the total amount of APO B is an indicator fairly accurate for estimating LDL-P (the total number of particles LDL). If the total amount of APO B is between 90-120 mg/dL, it is considered a good value (study, study). If it exceeds 140 mg/dL, the risk is very high: it means a lot of particles (smaller and with greater ability to pass through the endothelium). The APO B were measured by analysis of blood and is relatively cheap (between 10 and 20 €, depending on the lab). However, it is not usual to measure in Social Security. Once you know the APO B, the next step is to analyze the ratio LDL/APO B.
Ratio LDL/APO B (LAR, for its acronym in English)
We can have a low value of APO B because we have a LDL low, and this is also not positive. So a APO B under it is only desirable if the LDL is in its optimal range (110-150 mg/dL). To estimate the size of our particles, the ideal is to use the ratio LDL/APO B (LAR). The higher this ratio, the better (less APO B/particles for the same level of LDL = larger particles). If the LAR is less than 1.2, the particle size of LDL is approximately 25,5 nm or less (i.e., small and atherogenic). The optimum would be to keep it above 1.2 (study).
Summary
- Recent studies indicate that it is not necessary to keep the total cholesterol as low as possible; in fact, there is increased mortality from all causes by having it low to keep it high, according to the ranges of existing health services.
- Cholesterol is a type of fat that, to circulate in the blood, you need to bind to proteins, forming lipoproteins. According to its density (to a greater or lesser amount of fat/protein), there are several types of lipoproteins, but the two that most interest to us are the LDL and HDL.
- LDL carries cholesterol to the cells for use, while the HDL picks up excess, and takes it to the liver for recycling.
- We measured the cholesterol because what really interests us is to know our cardiovascular risk. However, neither total cholesterol nor LDL cholesterol total, which are measured in the analysis we provide a lot of information about it.
- The most important thing is to know the size of our LDL particles, since only the small size —once rusted and with the endothelium damaged by habits and unhealthy environments— have the ability to form the atherosclerotic plaque, which is responsible for cardiovascular problems.
- The methods to know the size of the particles LDL are expensive and not completely accurate. The best indirect way of obtaining this information is by measuring APO B (a method of economic and reliable), and then using the ratio LDL/APO B (LAR).